

Understanding Ebola: determinants, distribution, diagnosis, and drugs
Explore the critical aspects of Ebola, from its origins and global impact to its diagnostic methods and available treatments. Our goal is to provide clear, factual information for healthcare professionals, the general public, and students, fostering understanding without panic.

The African origins and impact of Ebola
Ebola is predominantly African in origin and impact. Its emergence and spread have deeply affected communities across the continent, highlighting the importance of understanding its roots and socio-economic determinants. This section delves into how the disease first appeared and its significant consequences for public health in affected regions.
A highly lethal disease: understanding its dangers
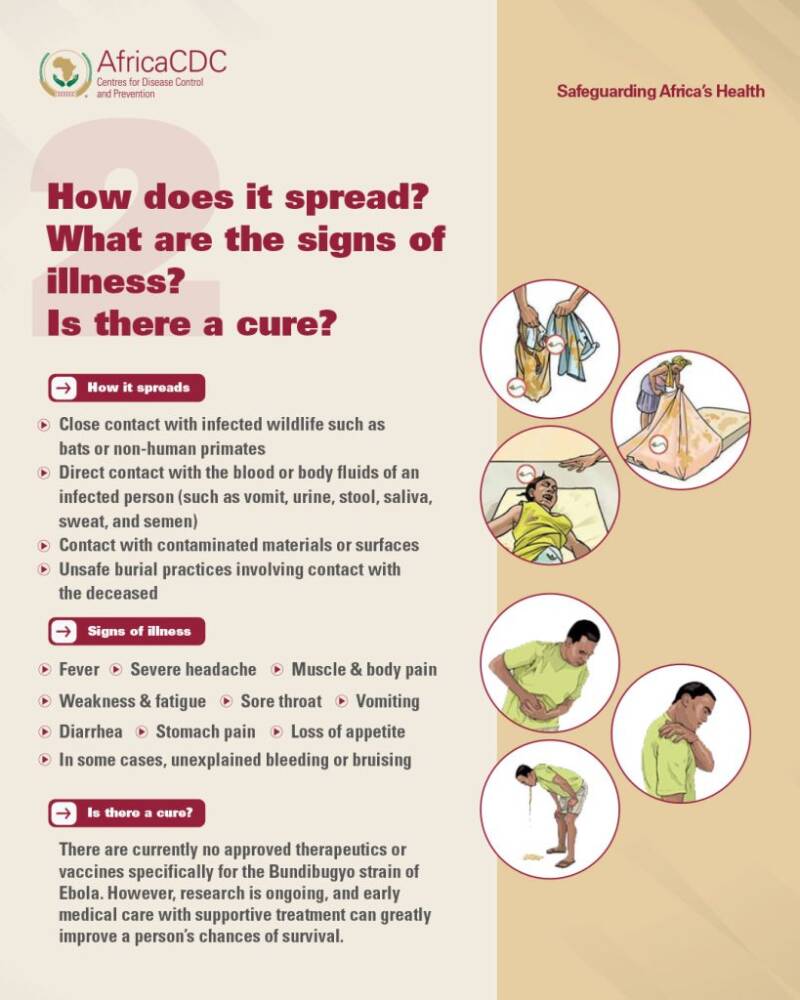
Ebola is known for its high lethality, making swift identification and intervention crucial. Learn about the severity of the disease, its modes of transmission, and the symptoms that indicate infection. This knowledge is vital for both preventing its spread and ensuring timely medical attention for those affected.

Ebola: a public health emergency of international concern
The Democratic Republic of Congo (DRC) outbreak of Ebola was declared a Public Health Emergency of International Concern by the WHO. This declaration underscores the global threat posed by Ebola and the need for coordinated international efforts in containment and response. Discover what this designation means for global health and the strategies employed to manage such outbreaks.
WHO Director-General's opening remarks at the media briefing – 24 June 2026

WHO Director-General's opening remarks at the media briefing – 24 June 2026
Good afternoon to those in the room, and good morning, good afternoon and good evening to those online, wherever you are in the world.
We begin with the Ebola outbreak in the Democratic Republic of the Congo.
It’s encouraging to see that since the outbreak was first reported five weeks ago, the response has scaled up significantly, under the leadership of the government.
In the past five weeks, the number of treatment beds has increased from less than 10 to over 500 in 19 health centres.
With support from WHO and the Africa CDC, laboratory capacity has increased from 30 tests a day at the central laboratory in Kinshasa to over 2000 tests a day in nine labs across three provinces.
More communities are becoming aware of the risks of Ebola, and asking for the tools and support to protect themselves.
And more than 100 people have now recovered. With early detection and supportive care, many can survive this disease.
But we could save many more lives with therapeutics.
Preparations are now complete for a trial of two therapeutics that is expected to start in DRC next week.
The trial will evaluate whether two antivirals, MBP134 and remdesivir, can help to reduce mortality in patients with Bundibugyo virus disease, alone or in combination.
We thank the United States and Gilead Sciences for donating doses for the trial. Together with our partners we will announce more information next week.
WHO and our partners are working closely with the communities to inform and involve them in the trial.
We are also working to ensure the communities have access to the therapeutics should they prove safe and efficacious.
The trial will be conducted by a consortium of partners including DRC’s National Institute for Biomedical Research, ALIMA, Oxford University and WHO.
Despite the good progress we have made, we still face major challenges, and the outbreak is continuing to outpace the response.
There are now 1094 confirmed cases, with 277 deaths.
The outbreak is continuing to move fast.
Political advocacy and action are essential to create the conditions for increased humanitarian access and a scaled-up response, because the outbreak is happening in a complex situation.
In neighbouring Uganda, a new case was reported last Sunday, the first in two weeks.
This brings the total in Uganda to 20 confirmed cases, with two confirmed deaths.
All cases in Uganda are linked to the outbreak in DRC.
Today, France reported that a health worker with the NGO ALIMA, who returned to the country after caring for an Ebola patient in DRC, tested positive for the virus, and is now being monitored and receiving care.
This case is a reminder of the risks faced by frontline responders.
Almost 80 health workers have been infected, highlighting the risks they face and the importance of strengthening infection prevention and control.
WHO advises countries to support the safe deployment of personnel responding to this outbreak.
This includes ensuring that organizations deploying staff provide clear information on risks, how to reduce and manage the risk of exposure, and that countries are prepared to facilitate evacuation if needed.
Still, the risk to the rest of the world remains low.
Under the government’s leadership, the coordinated response to the outbreak is starting to take hold.
But continued scale up is needed.
Contact tracing is still not at the level needed;
Capacity at treatment and isolation centres is insufficient;
Safe and dignified burials remain a major challenge;
The health system is under pressure;
Border closures continue to hinder the response;
Multiple security incidents have been reported;
The affected area is in the grip of a decades-long humanitarian crisis;
And financial support is still insufficient.
Earlier this month, WHO and the Africa CDC announced a joint Continental Preparedness and Response Plan that reflects the funding needs of partners, with an ask of 518 million U.S. dollars.
Next week, the first financial reporting on pledges and commitments to the plan are expected to be available, providing a clear understanding of gaps and needs.
===
Now to the outbreak of hantavirus.
The total number of cases from the hantavirus outbreak remains 13, including three deaths.
In all, more than 650 contacts have been identified and followed up by local health authorities in 33 countries and territories.
All but 54 contacts have completed their period of quarantine, and the remaining contacts are scheduled to complete their quarantine period by the 2nd of July.
If no further cases are reported by then, WHO will consider the outbreak to be over.
However, WHO will continue working to advance our understanding of this outbreak, and hantavirus more generally.
Working with governments and partners, we are continuing investigations into how the outbreak started and spread among those on board.
We are also working with partners who have collected environmental samples onboard the ship.
In addition, we are coordinating a study among people exposed to the virus involving 21 countries, to better understand how the disease develops.
We are also working on having a sample of the virus shared with the WHO BioHub in Switzerland.
This will be important for developing diagnostics, therapeutics and vaccines for future outbreaks.
I thank all countries that have contributed in different ways to the response to this outbreak, with special thanks to the leadership and solidarity shown by Spain, especially to Prime Minister Pedro Sánchez.
I also thank the Captain of the MV Hondius, Captain Jan Dobrogowski, his crew and all passengers for their cooperation in what has been a very difficult situation.
===
Now to the ongoing conflict in Sudan.
In the city of El Obeid in North Kordofan, the humanitarian situation continues to worsen.
WHO echoes concerns raised by the UN Security Council over the imminent risk of mass atrocities, and supports the demand for an immediate halt to assaults.
In neighbouring West Kordofan, the State Ministry of Health has reported 734 suspected cholera cases and 105 deaths, since the 15th of May.
The outbreak is occurring in the context of health systems disrupted by long-running conflict.
WHO and partners are responding to the outbreak by strengthening access to safe water and sanitation, establishing cholera treatment centres, prepositioning rapid diagnostic tests and medicines, and dispatching samples to South Sudan for testing.
===
Finally, countries across Europe and the northern hemisphere are experiencing an extreme heat wave.
Extreme heat is one of the most serious and rapidly growing threats to health and safety posed by climate change.
It claims around half a million lives globally each year, yet many of these deaths are preventable.
Heat affects everyone, but those at highest risk include older adults, people with chronic conditions, children, pregnant women, workers exposed to extreme heat, and socially disadvantaged populations.
Heatwaves can also become a major health hazard for people attending mass gatherings and sporting events.
During the World Cup, WHO is collaborating with FIFA and host countries on a “Beat the Heat initiative”, to develop action plans, raise awareness, establish early warning systems, improve access to safe drinking water, and implement cooling strategies and smart planning.
Fans, workers, and event organisers are all exposed to heat. Protecting them sends a powerful signal: health must be at the centre of global events.
Christian, back to you.

Saturday, 13 June 2026
Disease Outbreak News
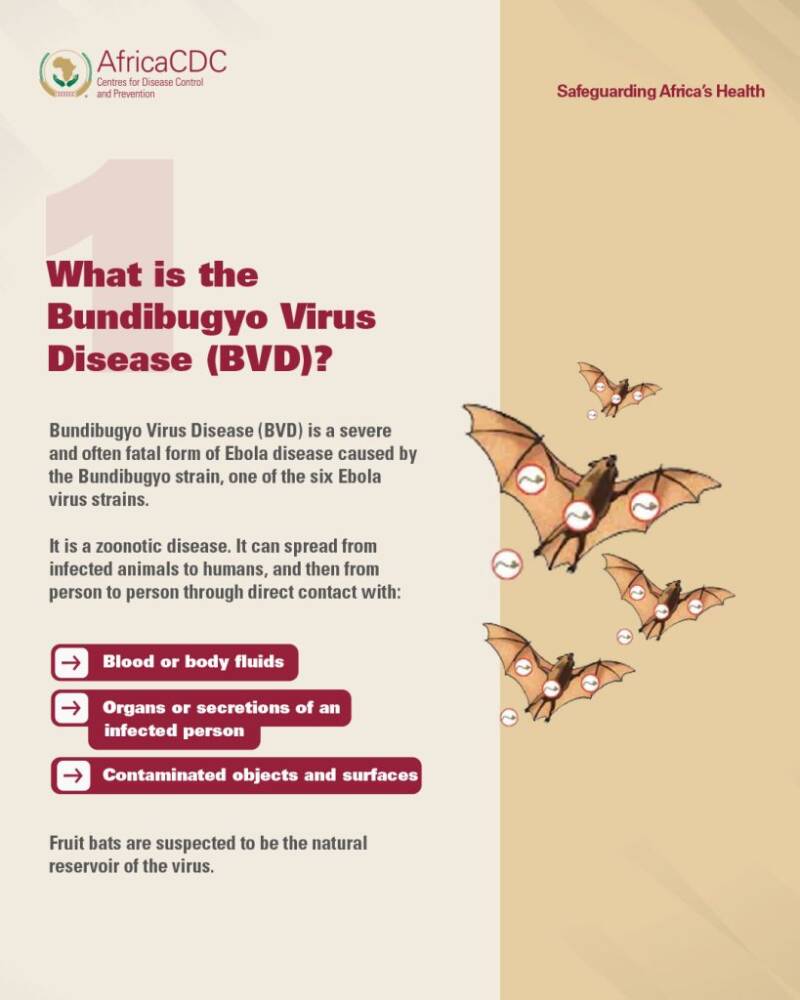
Ebola disease caused by Bundibugyo virus, Democratic Republic of the Congo & Uganda
Situation at a glance
The Bundibugyo virus disease (BVD) outbreak in the Democratic Republic of the Congo continues to evolve rapidly, with increasing case numbers and geographic spread. As of 10 June, a cumulative of 676 confirmed cases, including 136 deaths, have been reported from the Democratic Republic of the Congo. As of 11 June, Uganda has reported 19 confirmed cases including two deaths, as well as one probable case who has died. In Uganda, the outbreak remains epidemiologically linked to transmission originating in the Democratic Republic of the Congo, with evidence of both imported infections and secondary transmission among contacts and healthcare workers. Uganda has not reported any new cases in the past six days. National authorities in the two affected countries, in collaboration with WHO and partners, are implementing a comprehensive package of response measures. A regional preparedness and prioritization framework continues to guide readiness activities across the African Region.
The full text of the DON can be accessed here.
For further information, please also see:
See all DONs related to this event

WHO Director-General's opening remarks at the launch of the joint Bundibugyo Ebola virus continental strategic preparedness and response plan – 5 June 2026
Dr Jean Kaseya, Director-General of the Africa CDC,
Dr Mohamed Yakub Janabi, WHO Regional Director for Africa,
Dear colleagues, partners and friends from the media,
Good morning, good afternoon and good evening, and thank you for joining us.
Earlier this week, I returned from DRC, where I travelled to the epicentre of the Ebola outbreak in the province of Ituri.
I saw and heard first-hand the challenges that the communities are facing, and that the government and partners are facing, as we race to control this outbreak as quickly as possible.
The outbreak is moving fast, and we are still playing catch-up.
But my trip to the DRC also gave me real hope that together, under the government’s leadership, we can bring this outbreak under control.
The only way we will do that is through government leadership, community ownership and close partnership between the many actors on the ground.
Today, WHO and Africa CDC are expressing that partnership by launching a joint continental preparedness and response plan.
The objective is straightforward: we need to stop the outbreak where it is, support countries that are responding today, and ensure that neighbouring countries are ready to detect and act quickly if cases appear.
There are several important features of this plan.
First, it’s a shared plan. The only way to beat this outbreak is through close partnership, working together under the leadership of the affected countries in one coordinated effort, guided by a simple principle: one plan, one budget, one team.
Second, this is a practical plan. It sets out what we need to do now, together, to contain the current outbreak and reduce the risk of further spread.
Third, it’s a time-bound plan, covering June to November this year.
And fourth, it’s a costed plan, at US$ 518 million.
That figure represents the combined effort of WHO, Africa CDC and key partners including UNICEF, UNHCR, WFP, the IFRC and FIND.
Africa CDC and WHO are also establishing a joint financial tracking mechanism to monitor funding needs, commitments and gaps.
The plan focuses on core areas: emergency coordination, surveillance, laboratory testing, infection prevention and control, clinical care, and community engagement.
It also provides for research, logistics, and the continuity of essential health services, which are often disrupted during outbreaks.
Experience shows that success depends on how well these elements function together.
Surveillance must lead quickly to testing. Testing must trigger isolation and care;
Infection prevention must protect health workers and patients;
And community engagement must be continuous, grounded in trust, and responsive to concerns.
This plan builds directly on national response plans in the DRC and Uganda, where authorities are intensifying efforts to bring the outbreak under control.
It also supports preparedness in neighbouring countries, where cross-border movement creates ongoing risk.
WHO is engaged at all three levels to support the response.
But technical work alone is not enough. Containing Ebola depends on political commitment, sustained financing, and the trust and engagement of communities.
This plan places communities at the centre, because without their participation, contact tracing falters, safe care is delayed, and transmission continues.
Misinformation is almost as dangerous as the virus itself, and spreads just as fast.
Earning and keeping the trust of communities is at the heart of everything we do.
We are not starting from zero. This plan draws on lessons from previous Ebola outbreaks and recent health emergencies.
Those lessons are clear: speed matters, coordination matters, and consistency matters.
The opportunity now is to act with clarity and discipline, using a common plan to guide a common effort.
If we do that, we can bring this outbreak to an end and strengthen the systems that protect people from the next one.
This is a serious outbreak and it’s one we know how to stop but we need to move fast and together.
No country faces this alone.
As I said earlier, the key to this plan is partnership, especially between the Africa CDC and WHO.
I’m therefore pleased to invite the Director-General of the Africa CDC, Dr Jean Kaseya, to say a few words.
Jean, over to you.

Sunday, 31 May 2026
Joint statement by the Government of the Democratic Republic of the Congo and the World Health Organization concerning the outbreak of Ebola disease caused by the Bundibugyo virus
Bunia, 31 May 2026 – The Government of the Democratic Republic of the Congo (DRC) and the World Health Organization (WHO) reaffirm their strong partnership and shared commitment to protect the health and well-being of the people of Ituri Province and the nation at large, following the joint mission to Bunia led by Dr Samuel Roger Kamba, Minister of Health, Mr Patrick Muyaya Katembwe, Minister of Communication and Medias, and the visit of WHO Director-General Dr Tedros Adhanom Ghebreyesus.
This high-level visit comes at a challenging time, as the country responds to an outbreak of Ebola disease caused by the Bundibugyo virus. The Ministry of Health reports a rapidly evolving situation, with cases and deaths notified in several health zones of Ituri, North Kivu and South Kivu. The Government, with support from WHO and partners, is intensifying surveillance, laboratory testing and patient care to interrupt transmission as quickly as possible.
The Government of the DRC is firmly leading a comprehensive national response, working closely with provincial authorities in Ituri and neighbouring provinces. WHO, alongside the broader United Nations system and health and humanitarian partners, is fully committed to supporting these efforts. Together, DRC authorities, WHO and partners are working to strengthen coordination, mobilize additional resources, and ensure that life-saving interventions reach affected communities quickly and equitably.
Central to this response is the recognition that communities are at the heart of the solution. Success will depend on the trust, engagement and leadership of local communities. National and provincial authorities, with support from WHO and partners, are intensifying dialogue with community leaders, women's groups, youth representatives, religious leaders and the private sector to better understand local concerns and co-develop solutions that are culturally appropriate and effective.
While the Bundibugyo strain presents additional challenges, including the absence of a licensed vaccine or specific treatment, proven public health measures remain effective in slowing transmission and potential full recovery. The Ministry of Health, WHO and partners are working to rapidly undertake randomized control trials on candidate vaccines and treatments.
Persistent challenges include early detection and isolation of cases, contact tracing, safe and dignified burials, robust infection prevention and control in health facilities, and strong community awareness. The Government and WHO call on all communities to continue adopting protective behaviours, including regular hand hygiene, early care seeking in health facilities, and sharing accurate information.
The DRC brings unparalleled experience to this response, having successfully contained multiple previous Ebola outbreaks. This experience, combined with strong political leadership at the highest level of the State and renewed international solidarity, provides a firm foundation for bringing the current outbreak under control.
Both parties emphasize that outbreak response must maintain primary healthcare and essential services and strengthen long-term health system resilience. Investments made today in laboratories, health workers, surveillance systems and essential services will leave a legacy for the people of Ituri and the DRC as a whole.
The Government of the DRC is firmly leading a comprehensive national response, working closely with provincial authorities in Ituri and neighbouring provinces. WHO, alongside the broader United Nations system and health and humanitarian partners, is fully committed to supporting these efforts.
We sincerely thank our international partners for the support already provided to response operations, and we encourage sustained solidarity to bring this outbreak under control. Cooperation between countries must also ensure that borders remain open, and that entry controls do not obstruct the flow of desperately needed medical supplies and personnel.
Together, DRC authorities, WHO, Africa CDC and partners are working to strengthen coordination, mobilize additional resources, and ensure that life-saving interventions reach affected communities quickly and equitably.
./.
Related links
- Joint statement by the Government of the Democratic Republic of the Congo and WHO concerning the outbreak of Ebola disease caused by the Bundibugyo virus
- WHO Director-General's remarks at the press briefing on the Bundibugyo Ebola outbreak – 30 May 2026
- Ebola outbreak in the Democratic Republic of the Congo and Uganda
- WHO's work on Ebola disease
- Ebola disease
- Disease Outbreak News of 29 May 2026
- Photography: WHO Photo Library
- B-Roll: Opening of WHO/DRC Ebola Treatment Centre
WHO / DRC EBOLA TREATMENT CENTRE | UNifeed
High-level ministerial meeting on cross-border coordination on the Ebola disease outbreak caused by Bundibugyo virus


High-level ministerial meeting on cross-border coordination on the Ebola disease outbreak caused by Bundibugyo virus
COMMUNIQUÉ
Kampala, Republic of Uganda - WE, the Ministers of Health of the Democratic Republic of the Congo (DRC), the Republic of Uganda, and the Republic of South Sudan, together with Heads of Delegations, representatives of the Africa Centres for Disease Control and Prevention (Africa CDC), the World Health Organization (WHO), UNICEF, and development and technical partners, convened at the High-Level Ministerial Meeting on Cross-Border Coordination on the Ebola Disease Outbreak caused by Bundibugyo virus held in Kampala, Uganda, from 22–23 May 2026 under the theme: "Regional Solidarity, Preparedness and Coordinated Response.
PREAMBLE
MINDFUL that Ebola disease remains a high-consequence public health threat with severe health, humanitarian, social, and economic implications for affected countries and the region;
CONCERNED by the evolving Bundibugyo virus disease (BVD) outbreak declared by the Government of the Democratic Republic of the Congo on 15 May 2026, following laboratory confirmation of the Bundibugyo species in Ituri province;
NOTING with concern the epidemiological situation as of 20 May 2026, including confirmed transmission in Ituri and Nord-Kivu provinces, increasing numbers of suspected and confirmed cases, ongoing chains of transmission, and documented cross-border population movement signals involving Uganda and the broader region;
NOTING that the current outbreak affecting and Kivu provinces constitutes both a Public Emergency of International Concern and a Public Health Emergency of Continental Security, requiring strengthened regional coordination and solidarity to urgently contain the outbreak and prevent further cross-border spread;
RECOGNISING the heightened regional risk associated with porous borders, active trade and mining corridors, humanitarian crises, population displacement, insecurity, and limitations in surveillance and preparedness capacities at points of entry and border communities;
ACKNOWLEDGING the efforts of the Governments of the DRC, Uganda and South Sudan, frontline health workers, rapid response teams, laboratory personnel, humanitarian actors, communities, and partners supporting the ongoing preparedness and response efforts;
RECALLING the obligations of Member States under the International Health Regulations (2005), the Africa CDC framework for regional collaboration and health security, and continental commitments toward strengthening epidemic preparedness, surveillance, and coordinated emergency response systems;
WELCOMING the leadership of Africa CDC and WHO in convening this High-Level Ministerial Meeting to strengthen regional solidarity, technical coordination, and operational preparedness and response to the Bundibugyo virus disease outbreak;
WE HEREBY agree on the following actions and commitments:
1. Strengthen Cross-Border Surveillance and Early Warning SystemsCommit to strengthening coordinated cross-border disease surveillance systems, event-based surveillance, joint contact tracing, active case finding, and real-time information sharing among the DRC, Uganda, and South Sudan, including routine cross-border coordination meetings and harmonised reporting mechanisms.
2. Harmonise Points of Entry Preparedness and Population Mobility MonitoringCommit to strengthening and harmonising public health measures at official and unofficial points of entry, including traveller screening, alert management, referral pathways, population mobility mapping, and monitoring along high-risk mobility corridors and border communities.
3. Protect Frontline and Vulnerable CommunitiesCommit to prioritising the protection of frontline health workers, displaced populations, mining communities, border communities and other vulnerable populations disproportionately exposed to the risk of transmission.
4. Strengthen Community EngagementRecognise the central role of trusted community leaders, civil society, media and local networks in promoting public awareness, early detection, prevention measures and community trust during outbreak response operations.
5- Strengthen Laboratory Systems and Diagnostic CapacityCommit to strengthening laboratory preparedness through decentralised diagnostic capacity, rapid sample transportation systems, genomic sequencing, surge staffing, and interoperability of laboratory information systems to support timely confirmation and response.
5. Strengthen Clinical Management and Infection Prevention and ControlCommit to strengthening case management capacity, triage systems, Infection Prevention and Control (IPC), Water, Sanitation and Hygiene (WASH), isolation capacity, safe and dignified burials, and protection of frontline healthcare workers in affected and at-risk areas.
6. Strengthen Risk Communication and Community EngagementCommit to strengthening Risk Communication and Community Engagement (RCCE) interventions, including community-based disease surveillance, social listening, rumour management, infodemic management, community feedback systems, and engagement of traditional, religious, youth, women, and local leaders to improve trust, acceptance, and adherence to public health measures.
7. Strengthen Operational Coordination and Incident ManagementSupport the operationalisation and strengthening of the Africa CDC Continental Incident Management Support Team (IMST), Emergency Operations Centres (EOCs), and national and sub-national coordination mechanisms to ensure harmonised regional preparedness and response operations.
8. Mobilise Sustainable Financing and Operational SupportCall upon Member States, regional institutions, development partners, humanitarian actors, donors, and the private sector to urgently mobilise and align financial, technical, logistical, and operational support behind national preparedness and response plans, including support for surveillance, laboratory systems, RCCE, IPC, and workforce surge capacity.
9. Strengthen Regional Preparedness and Health SecurityCommit to strengthening preparedness capacities in at-risk countries and border districts, including simulation exercises, workforce development, stockpiling of critical supplies, rapid response readiness, and continuity of essential health services during the outbreak response.
10. Sustain High-Level Political Leadership and Regional SolidarityReaffirm our commitment to sustained political leadership, transparency, multisectoral collaboration, and regional solidarity to contain the outbreak, prevent regional spread, and protect the health security and socioeconomic stability of the region.
11. Advance Long-term Regional Health SecurityUnderscore the urgency of investing in resilient health systems, regional preparedness capacities, workforce development, laboratory networks and emergency coordination systems to strengthen Africa's collective health security and preparedness for future outbreaks.
12. Ensure the continuity of essential servicesThe critical maintenance of essential services includes healthcare, education, and other critical social services, in the affected provinces and countries throughout the response to the outbreak.
We express our appreciation to the Government and people of the Republic of Uganda for hosting this important meeting, and commend the efforts of frontline responders, health workers, communities and partners working tirelessly to contain the outbreak.
DONE in Kampala, Republic of Uganda, on 23 May 2026.
No images? Click here
Thursday, 28 May 2026
Message by the WHO Director-General to the people of the Democratic Republic of the Congo
English and Swahili: https://www.who.int/news/item/28-05-2026-message-by-the-who-director-general-to-the-people-of-the-democratic-republic-of-the-congo
To the people of DRC, especially to the people of Ituri
Jambo kwenu wakahaji wa Ituri
Mbote na bino, bato ya Ituri
My name is Tedros, and I am the Director-General of the World Health Organization (WHO). But today, I am not writing to you as an official. I am writing to you as someone who knows your region, who has walked your streets, and who cares deeply about what happens to you and your families.
I am writing because I want to be with you in these moments. And I want you to know that you are not alone.
Ebola is not new to me personally. From 2018 to 2020, I came fourteen times to North Kivu, the epicentre of the outbreak at that time. Fourteen visits to Beni, Butembo, Katwa, Goma, and many other communities. During that outbreak, Ebola spread across North Kivu, South Kivu, and reached parts of Ituri as well. I was alongside families who had lost their loved ones. I met health workers risking their lives every day. I met community leaders, traditional healers, religious leaders and business leaders who refused to abandon their people. I saw men and women show extraordinary courage in the most difficult of circumstances. The people there, who saw me coming back again and again, wanted to give me a name that belonged to their community. They asked me whether I was the first, second, or third child of my parents. When I told them I was the firstborn, they gave me the name Dr. Paluku. I carry that name with pride. It is not just a name. It is a bond. It is a reminder that this work is not about titles or institutions. It is about people. It is about you.
That outbreak was one of the most complex in history. It did not unfold in a stable, peaceful environment. It happened in the middle of armed conflict, with communities displaced, supply routes disrupted, and health workers operating under constant threat. People were fleeing violence while also trying to protect themselves and their families from a deadly disease. I remember being in Beni on more than one occasion while fighting was taking place on the outskirts of the city. We could hear it. And yet the health workers around me did not stop. They kept working. That kind of courage is something I will never forget. The challenges of that time are not so different from what you are facing today in Ituri. I understand that. I have seen it with my own eyes.
Mistrust ran deep, and the security situation cost us precious time. Our health workers were attacked. Clinics were targeted. People who were only trying to save lives found themselves caught in the middle of a conflict they did not start. Lives were lost that we might have saved, and that weighs on me still. But I also witnessed something remarkable. When we listened, when communities felt respected and heard, things began to change. Trust grew slowly, then more quickly. People came forward. And together, we managed to contain the outbreak. We did it. The people of DRC did it. I will never forget that.
Ebola is now back. This time, the outbreak is hitting Ituri province the hardest. More than 90% of all cases have been reported in Ituri province, with a small number of cases also reported in North Kivu and South Kivu. I know how frightening that is, and I know that the people of Ituri are bearing a burden that is not easy to carry.
I know that many of you are exhausted. You are already carrying so much: malaria, hunger, insecurity, and the daily struggle to keep your families safe. And now Ebola. It is not fair, and I will not pretend otherwise.
But I also want to say something else about Ituri, because this province deserves to be seen for more than its hardships. Ituri is a place of remarkable energy. It is a province of vibrant commerce, of entrepreneurial spirit, of communities that have refused to be defined by the conflicts around them. The markets of Bunia buzz with life. Traders, farmers, teachers, and young people building their futures against all odds. That spirit, that refusal to give up, is exactly what we need now. It is the foundation on which we will build our response. We do not come to Ituri with only medicine and expertise. We come to join a community that already knows how to fight for its survival.
I want to say a special word to the young people of Ituri. You are growing up in circumstances that no young person should have to face. And yet what I see, again and again, is not despair but determination. You are the future of this province and this country. In this outbreak, you have a vital role to play. Talk to your friends and your families. Share what you know about Ebola. Help break the fear and the silence that allow this virus to spread. Your voice carries further than you know, and we need it now more than ever.
And to the health workers of Ituri, I want to say this: you are seen, and you are not alone. Every day you go to work knowing the risks, and you go anyway. You do it for your patients, for your communities, for your families. You are the backbone of this response. Without you, none of this is possible. I know the conditions are hard. I know the resources are often not enough. I know that fear and exhaustion are real. Please know that WHO stands with you, that we are working to get you the support you need, and that your courage and dedication are known and deeply valued far beyond the borders of this province.
I also know that the security situation in parts of this region remains very difficult. Conflict and displacement make everything harder, including reaching people who need care and keeping health workers safe. I want to be honest: this is one of our greatest challenges. We cannot do this work if those who are trying to help are prevented from doing so or put in danger. We are working closely with all relevant partners to ensure that the response can reach every community that needs it, and that no one is left behind because of where they live or what is happening around them.
That is why today I am making a direct appeal to all warring parties in this region: please, declare a ceasefire. Even briefly. Even just enough to let health workers through. People are dying from Ebola who do not have to die. Children are sick. Families are suffering. No cause, no conflict, no grievance is worth condemning innocent people to death from a preventable disease. A ceasefire, even a temporary one, would save lives. I urge you, I implore you: give us the space to help the people who need it most.
I also know that there is anger and mistrust in some communities, and I understand why. Trust must be earned, it cannot be assumed. We have not always done things correctly. But I promise you, we are here to learn as much as we are here to help.
I need to be honest with you about something important. Most previous Ebola outbreaks in DRC were caused by a virus called Ebola Zaire, for which we have vaccines and treatments. This outbreak is caused by a different virus called Ebola Bundibugyo. There are currently no approved vaccines or treatments for it. This is serious, and you deserve to hear that plainly. But I also want you to know this: while there are no specific treatments for Bundibugyo, there is much we can do together to prevent the spread of this virus and save lives. Early supportive care in our treatment centers can make a real difference. If you or someone you know falls ill, please do not wait. Coming forward early can make the difference between life and death. And everything we do, we will do with you. We will listen to you, we will share information with you, and we are here to help. And for those we cannot save, we will mourn with you. We will help you grieve your lost loved ones with safe and dignified burials.
We are working under the leadership of the Government of DRC, together with all relevant partners, united around one goal: to stop this outbreak and protect your communities. No one is working alone. No one is working at cross purposes. We are coordinated, we are committed, and we are here.
That is why I am coming to Bunia. I will be there in person, alongside my colleagues, meeting your leaders, listening to your concerns, and doing everything in my power to help you. I will not be managing this from a comfortable office far away.
This is the 17th Ebola outbreak in DRC. Together, you have overcome every single one before. That is not a small thing. That is a testament to the strength and resilience of your communities. I have seen that strength with my own eyes.
My brothers and sisters of Ituri, I want you to know that the world is watching your courage. You are not forgotten. Together, we will overcome this outbreak, as you have overcome every challenge before. Your resilience is the light that guides us all.
We will get through this one too. Not because of anyone, but because of you.
Our teams are already on the ground, and they will stay for as long as necessary. And when this outbreak is over, we will not quietly disappear. We will not forget you. We will stay, and we will keep working with you to build health systems that protect every person in every community.
I look forward to seeing you in Bunia soon. Until then, please know that you are in my thoughts.
With respect and solidarity,
Paluku
Tedros
Tedros Adhanom Ghebreyesus
Director-General, World Health Organization
****************
Kwa watu wa DRC, hasa kwa watu wa Ituri
Jambo kwenu wakahaji wa Ituri
Mbote na bino, bato ya Ituri
Jina langu ni Tedros, na mimi ni Mkurugenzi Mkuu wa Shirika la Afya Duniani (WHO). Lakini leo, siandikii kama afisa. Ninaandika kama mtu anayejua mkoa wenu, aliyetembea barabarani kwenu, na anayejali kwa moyo wote kinachowapata ninyi na familia zenu.
Ninaandika kwa sababu nataka kuwa nanyi katika nyakati hizi. Na nataka mjue kwamba hamko peke yenu.
Ebola si mgeni kwangu kibinafsi. Kuanzia mwaka 2018 hadi 2020, nilifika mara kumi na nne Kivu ya Kaskazini, kitovu cha mlipuko wakati huo. Ziara kumi na nne kwa Beni, Butembo, Katwa, Goma, na katika makundi mengi mengine. Wakati wa mlipuko huo, Ebola ilienea katika Kivu ya Kaskazini, Kivu ya Kusini, na kufikia sehemu za Ituri pia. Nilikuwa pamoja na familia zilizopoteza wapendwa wao.
Nilikutana na wafanyakazi wa afya wakihatarisha maisha yao kila siku. Nilikutana na viongozi wa jamii, waganga wa jadi, viongozi wa kidini na viongozi wa biashara ambao walikataa kuacha watu wao. Niliona wanaume na wanawake wakionyesha ujasiri wa kipekee katika mazingira magumu zaidi. Watu wale, walioniona
nikirudi tena na tena, walitaka kunipa jina lililokuwa la jamii yao. Waliniuliza kama mimi ni mtoto wa kwanza, wa pili, au wa tatu kwa wazazi wangu.
Nilipowaambia kuwa mimi ni mzaliwa wa kwanza, walinipa jina la Dkt. Paluku. Ninabeba jina hilo kwa fahari. Si jina tu. Ni kifungo. Ni ukumbusho kwamba kazi hii haihusu vyeo au taasisi. Inahusu watu. Inahusu ninyi.
Mlipuko ule ulikuwa miongoni mwa migumu zaidi katika historia. Haukutokea katika mazingira ya utulivu na amani. Ulitokea katikati ya vita vya silaha, na jamii zikiwa zimehamishwa, njia za usambazaji zikivurugwa, na wafanyakazi wa afya wakifanya kazi chini ya tishio la kudumu. Watu walikimbia ukatili huku wakijaribu kujikinga wao wenyewe na familia zao dhidi ya ugonjwa mbaya. Ninakumbuka kuwepo Beni zaidi ya mara moja wakati mapigano yalifanyika pembezoni mwa mji. Tuliweza kuyasikia. Na bado wafanyakazi wa afya waliokuwa karibu nami hawakusimama. Waliendelea kufanya kazi. Ujasiri kama huo ni kitu ambacho sitasahau kamwe. Changamoto za wakati huo si tofauti sana na mnazokabiliwa nazo leo Ituri. Naelewa hilo. Nimeshuhudia kwa macho yangu mwenyewe.
Kutokuamini kulikuwa kwa kina, na hali ya usalama iligharikimu muda wa thamani.
Wafanyakazi wetu wa afya walishambuliwa. Vituo vya afya viliwekwa lengo. Watu
waliokuwa tu wakijaribu kuokoa maisha walijikuta katikati ya mgogoro ambao
hawakuuanzisha. Maisha yalipotea ambayo tungeweza kuokoa, na hilo bado
linanisumbua. Lakini pia nilishuhudia kitu cha ajabu. Tulipoweza kusikiliza, jamii zilipohisi kuheshimiwa na kusikizwa, mambo yalianza kubadilika. Imani iliongezeka polepole, kisha haraka zaidi. Watu walijitokeza. Na pamoja, tuliweza kudhibiti mlipuko. Tulifanya hivyo.
Watu wa DRC walifanya hivyo. Sitasahau kamwe.
Sasa Ebola imerudi. Wakati huu, mlipuko unaikumba mkoa wa Ituri zaidi ya yote. Zaidi ya asilimia 90 ya visa vyote vimeripotiwa katika mkoa wa Ituri, na idadi ndogo ya visa pia vikiripotiwa Kivu ya Kaskazini na Kivu ya Kusini. Najua jinsi hilo linavyotisha, na najua kwamba watu wa Ituri wanabeba mzigo ambao si rahisi kubeba.
Najua kwamba wengi wenu mmechoka. Mnabeba mengi tayari: malaria, njaa, kutokuwa na usalama, na mapambano ya kila siku ya kuweka familia zenu salama. Na sasa Ebola. Si haki, na sitadanganya vinginevyo.
Lakini pia nataka kusema jambo lingine kuhusu Ituri, kwa sababu mkoa huu unastahili kuonekana kwa zaidi ya matatizo yake. Ituri ni mahali pa nishati ya ajabu. Ni mkoa wenye biashara inayosisimua, roho ya ujasiriamali, na jamii ambazo zimekataa kufafanuliwa na migogoro inayozizunguka. Masoko ya Bunia yanafurika uhai. Wafanyabiashara, wakulima, walimu, na vijana wanaojenga mustakabali wao dhidi ya vikwazo vyote. Roho hiyo, kukataa kukata tamaa, ndiyo hasa tunachohitaji sasa. Ndiyo msingi ambao juu yake tutajenga jibu letu. Hatukuja Ituri na dawa na ujuzi peke yake. Tumekuja kujiunga na jamii inayojua tayari jinsi ya kupigana kwa ajili ya uhai wake.
Nataka kusema neno maalum kwa vijana wa Ituri. Mnakua katika hali ambazo hakuna kijana anayepaswa kukabiliwa nazo. Na bado ninachokiona, tena na tena, si kukata tamaa bali uamuzi imara. Ninyi ndio mustakabali wa mkoa huu na nchi hii. Katika mlipuko huu, mna jukumu muhimu la kucheza. Zungumzeni na marafiki zenu na familia zenu. Shiriki unachojua kuhusu Ebola. Saidia kuvunja hofu na ukimya unaouruhusu virusi hivi kuenea.
Sauti yenu inasikika mbali zaidi kuliko mnavyofikiri, na tunaihitaji sasa zaidi ya wakati wowote.
Na kwa wafanyakazi wa afya wa Ituri, nataka kusema hivi: mnaonekana, na hamko peke yenu. Kila siku mnakwenda kazini mkijua hatari, na mnakwenda hata hivyo. Mnafanya hivyo kwa ajili ya wagonjwa wenu, kwa ajili ya jamii zenu, kwa ajili ya familia zenu. Ninyi ndio uti wa mgongo wa jibu hili. Bila ninyi, hakuna kitu chochote kinachowezekana. Najua hali ni ngumu. Najua rasilimali mara nyingi hazitoshi. Najua hofu na uchovu ni wa kweli. Tafadhali jueni kwamba WHO inasimama pamoja nanyi, kwamba tunafanya kazi kupata msaada
unaohitajika, na kwamba ujasiri wenu na kujitolea kwenu vinajulikana na kuthaminiwa sana mbali zaidi ya mipaka ya mkoa huu.
Pia najua kwamba hali ya usalama katika sehemu za mkoa huu inabaki kuwa ngumu sana. Migogoro na uhamishaji hufanya kila kitu kuwa kigumu zaidi, ikiwa ni pamoja na kuwafikia watu wanaohitaji huduma, na kuweka wafanyakazi wa afya salama. Nataka kuwa mkweli: hii ni moja ya changamoto zetu kubwa zaidi. Hatuwezi kufanya kazi hii kama wale wanaojaribu kusaidia wanazuiwa kufanya hivyo, au kuwekwa katika hatari. Tunafanya kazi kwa karibu na washirika wote wanaohusika kuhakikisha kwamba jibu linaweza kufikia kila jamii inayohitajika, na kwamba hakuna anayeachwa nyuma kwa sababu ya mahali wanapoishi au kinachoendelea karibu nao.
Ndiyo maana leo ninafanya ombi la moja kwa moja kwa pande zote zinazopigana katika mkoa huu: tafadhali, tangaza kusimama kwa mapigano. Hata kwa muda mfupi. Hata kiasi cha kuwaruhusu wafanyakazi wa afya kupita. Watu wanakufa kutokana na Ebola ambao
hawahitaji kufa. Watoto wanaugua. Familia zinateseka. Hakuna sababu, hakuna mgogoro, hakuna malalamiko yanayostahili kuwahukumia watu wasio na hatia kifo kutokana na ugonjwa unaoweza kuzuiwa. Kusimama kwa mapigano, hata kwa muda, kutaokoa maisha.
Nawasihi, nawaomba kwa nguvu zote: tupeni nafasi ya kusaidia watu wanaohitajika zaidi.
Pia najua kwamba kuna hasira na kutokuamini katika baadhi ya jamii, na naelewa kwa nini.
Imani lazima ipatikane, haiwezi kudhaniwa. Hatujafanya mambo vizuri kila wakati. Lakini ninaahidi, tuko hapa kujifunza kama vile tupo hapa kusaidia.
Ninahitaji kuwa mkweli nawe kuhusu jambo muhimu. Milipuko mingi ya awali ya Ebola nchini DRC ilisababishwa na virusi viitwavyo Ebola Zaire, ambavyo tuna chanjo na matibabu. Mlipuko huu unasababishwa na virusi tofauti viitwavyo Ebola Bundibugyo. Kwa sasa hakuna chanjo wala matibabu yaliyoidhinishwa dhidi yake. Hii ni mbaya, na mnastahili kusikia hilo wazi. Lakini pia nataka mjue hivi: ingawa hakuna matibabu maalum ya Bundibugyo, kuna mengi tunayoweza kufanya pamoja kuzuia kuenea kwa virusi hivi na kuokoa maisha. Huduma ya msaada wa mapema katika vituo vyetu vya matibabu inaweza kuleta tofauti ya kweli. Kama wewe au mtu unayemjua anaugua, tafadhali usisubiri.
Kujitokeza mapema kunaweza kumaanisha tofauti kati ya maisha na kifo. Na kila
tunachofanya, tutafanya nawe. Tutakusikiliza, tutashiriki taarifa nawe, na tuko hapa kukusaidia. Na kwa wale ambao hatuwezi kuwaokoa, tutaomboleza nawe. Tutakusaidia kuomboleza wapendwa wako waliopotea kwa mazishi salama na yenye heshima. Tunafanya kazi chini ya uongozi wa Serikali ya DRC, pamoja na washirika wote wanaohusika, tukiungana kwa lengo moja: kusimamisha mlipuko huu na kulinda jamii zenu. Hakuna anayefanya kazi peke yake. Hakuna anayefanya kazi kwa madhumuni tofauti.
Tunaratibishwa, tumejitolea, na tuko hapa.
Ndiyo maana ninakuja Bunia. Nitakuwepo mwenyewe, pamoja na wenzangu, nikutana na viongozi wenu, nikisikiliza wasiwasi wenu, na kufanya kila niwezalo kukusaidia.
Sitasimamia hili kutoka ofisi ya starehe mbali nawe.
Huu ni mlipuko wa 17 wa Ebola nchini DRC. Pamoja, mmeshinda kila mmoja wa milipuko iliyopita. Hilo si jambo dogo. Ni ushahidi wa nguvu na ustahimilivu wa jamii zenu.
Nimeshuhudia nguvu hiyo kwa macho yangu mwenyewe.
Ndugu zangu wa Ituri, nataka mjue kwamba dunia inaangalia ujasiri wenu.
Hamjasahauliwa. Pamoja, tutashinda mlipuko huu, kama vile mlivyoshinda kila
changamoto iliyopita. Ustahimilivu wenu ni nuru inayotuongoza sisi sote.
Tutapita pia wakati huu. Si kwa sababu ya mtu yeyote, bali kwa sababu yenu.
Timu zetu zipo tayari huko, na zitabaki kwa muda wote unaohitajika. Na mlipuko huu utakapokwisha, hatutaondoka kimya kimya. Hatutawasahau. Tutabaki, na tutaendelea kufanya kazi nanyi kujenga mifumo ya afya inayolinda kila mtu katika kila jamii.
Ninatazamia kuwaona Bunia hivi karibuni. Hadi hapo, tafadhali jueni kwamba mko katika mawazo yangu.
Kwa heshima na mshikamano,
Paluku
Tedros
Tedros Adhanom Ghebreyesus
Mkurugenzi Mkuu, Shirika la Afya Duniani
Saturday, 23 May 2026
Disease Outbreak News
Ebola disease caused by Bundibugyo virus - Democratic Republic of the Congo
21 May 2026
Situation at a glance
On 15 May 2026, the Ministry of Public Health, Hygiene and Social Welfare, Democratic Republic of the Congo (DRC), and the Ministry of Health of Uganda declared an outbreak of Ebola Disease following the confirmation of Bundibugyo virus disease (BVD) in both countries. On 16 May 2026, the World Health Organization (WHO) Director-General determined that the Ebola disease caused by Bundibugyo virus in DRC and Uganda constitutes a public health emergency of international concern (PHEIC), as defined in the provisions of IHR. On 19 May 2026, the Director-General of WHO convened the first meeting of the IHR Emergency Committee, and temporary recommendations were issued to State Parties. As of 21 May, 746 suspected cases and 176 deaths among suspected cases were reported in DRC. So far 85 confirmed cases, including two in Uganda, and ten deaths, with one in Uganda, among confirmed cases were reported across both countries. In DRC, transmission is concentrated in Ituri, North Kivu and South Kivu provinces, with challenges in contact follow-up, insecure conditions, and inadequate isolation and referral systems complicating response efforts. Uganda has reported two imported cases with no confirmed local transmission. An American national who was working in DRC has also been confirmed positive and transferred to Germany for care. National authorities, in collaboration with WHO and partners, are implementing response measures including deployment of rapid response teams, delivery of medical supplies, strengthened surveillance, laboratory confirmation, infection prevention and control assessments, the set-up of safe and optimized treatment centers, and community engagement.
The full text of the DON can be accessed here: Ebola disease caused by Bundibugyo virus – Democratic Republic of the Congo
For further information, please also see:
Thursday, 28 May 2026
NEWS RELEASE
Experts convened by WHO advise on candidate treatments and vaccines for Ebola disease caused by Bundibugyo virus
Geneva, 28 May 2026 -- In response to the current outbreak of Ebola disease caused by Bundibugyo virus occurring in the Democratic Republic of the Congo, with cases also reported in Uganda, WHO convened several of its expert and advisory groups. These groups assessed potential vaccines and therapeutics for both prevention and treatment of Bundibugyo virus disease (BVD). The WHO advisory groups recommended that all the products identified and considered be used exclusively within clinical trials to generate robust data and ensure safe, ethical, and effective research.
WHO convened a series of meetings with the WHO R&D Blueprint technical advisory groups on candidate vaccines and therapeutics for BVD.
In parallel, WHO also convened the Strategic Advisory Group of Experts on Immunization (SAGE) and its Ebola vaccine working group to advise on the potential role of licensed Ebola vaccines during BVD outbreaks.
Key recommendations
There are currently no licensed therapeutics or vaccines specifically approved for the prevention and treatment of BVD. Nevertheless, WHO advisory groups considered several candidate products that are promising enough to warrant prioritization for evaluation in clinical trials. WHO is now working closely with the governments of the Democratic Republic of the Congo and Uganda to facilitate the implementation of research evaluation of these products.
For treatment of cases:
- For treatment, the independent experts recommended prioritizing three candidate therapeutics for evaluation in research (i.e. clinical trials) among confirmed BVD cases: the monoclonal antibodies MBP134 and Maftivimab®, as well as the antiviral remdesivir.
- Combination therapy using a monoclonal antibody and remdesivir is also recommended for evaluation.
For prevention of cases:
- For post-exposure prophylaxis among contacts of confirmed and probable cases, the oral antiviral obeldesivir was determined to be a priority candidate, although experts noted that this approach depends on effective contact tracing, which remains operationally challenging in some of the affected areas of the Democratic Republic of the Congo. Research on post-exposure prophylaxis involves giving tablets of obeldesivir to contacts of cases to evaluate whether this prevents them from developing Ebola disease.
- The most promising candidate vaccine was determined by the experts to be the single-dose rVSV Bundibugyo vaccine (being developed by the International AIDS Vaccine Initiative or IAVI). The development of this single-dose vaccine candidate will likely require 7–9 months before it is ready to be assessed through a clinical trial for its ability to prevent BDV.
- Another candidate vaccine, ChAdOx1 Bundibugyo (being developed by Oxford University/Serum Institute of India) could potentially become available within 2–3 months for efficacy assessment through a clinical trial. However, additional animal data are still required to support and confirm further prioritization. Experts noted that a single-dose vaccine approach of this candidate could be suitable for contacts of Ebola cases, whereas a two-dose strategy might be considered for high-risk but unexposed populations such as health-care workers and frontline responders.
- The convened experts also reviewed the potential role of Ervebo, the only licensed Ebola vaccine. It is approved for use during outbreaks caused by the most common Ebola virus in Africa, from the Orthoebolavirus family. Ervebo is not licensed for prevention of BVD and evidence on cross-protection to other Ebola virus species remains limited and inconclusive. WHO recommends that Ervebo should not be used outside carefully designed research settings, to allow for its performance against BDV to be assessed.
Ensuring ethical and safe clinical trials
WHO, the governments of the Democratic Republic of the Congo and Uganda, the Africa Centres for Disease Control and Prevention (Africa CDC), the ANRS Emerging infectious diseases (French National Agency for Research on AIDS and Viral Hepatitis), and other scientific partners are working together to develop and implement appropriate protocols to assess the safety and efficacy of the prioritized therapeutics through clinical field trials.
WHO calls for accelerated access to essential supplies, stronger community protection, engagement and trust, and coordinated investment in the research, development and evaluation of BVD countermeasures.
All research must adhere to the highest ethical standards, under the leadership of the national health authorities and in close consultation with affected communities.
In the meantime, our priority is to stop transmission with tools that we have used for decades of Ebola responses, which include disease surveillance, rapid testing and diagnosis, contact tracing, isolation and care for patients, infection prevention and control, community engagement, and safe and dignified burials.
Background
The WHO R&D Blueprint is a global initiative that allows the rapid activation of research and development activities during epidemics. Its aim is to fast-track the availability of proven effective tests, vaccines, and medicines that can be used to save lives and avert large-scale crises.
SAGE is the principal advisory group to WHO for vaccines and immunization. It is charged with advising WHO on overall global policies and strategies, ranging from vaccines and technology, research and development, to delivery of immunization and its linkages with other health interventions.
About WHO
Dedicated to the well-being of all people and guided by science, the World Health Organization leads and champions global efforts to give everyone, everywhere an equal chance at a safe and healthy life.
We are the UN agency for health that connects nations, partners and people on the front lines in 150+ locations – leading the world’s response to health emergencies, preventing disease, addressing the root causes of health issues and expanding access to medicines and health care. Our mission is to promote health, keep the world safe and serve the vulnerable.
“Together for health. Stand with science”, the theme of World Health Day 2026 marks a year-long campaign to highlight science as the foundation for protecting health and well-being worldwide.
Links:
- WHO Technical Advisory Group on therapeutics prioritization for Bundibugyo virus disease: meeting report, 20 and 26 May 2026
- WHO Technical Advisory Group on candidate vaccine prioritization: meeting report, 19 and 25 May 2026
- WHO emergency guidance on the use of licensed Ebola virus vaccine during Bundibugyo virus disease outbreaks, 28 May 2026
- WHO R&D blueprint
- SAGE working group
- WHO Ebola outbreak in DRC emergency webpage
- WHO Ebola disease fact sheet
WHO Director-General's remarks at the Virtual Ministerial Briefing on the Bundibugyo Ebola Outbreak – 25 May 2026
Organizers: Africa CDC
25 May
Your Excellency President Cyril Ramaphosa,
Thank you so much for your leadership, and for announcing the financial contribution, which is important for Africa CDC.
Your Excellency Chairperson Mahmoud Ali Youssouf,
Honourable Minister Khaled Abdel Ghaffar,
Africa CDC Director-General Dr Jean Kaseya,
Dear colleagues and friends,
I thank President Ramaphosa and Chairperson Youssouf for their leadership, and I thank my brother Dr Jean Kaseya for convening this briefing.
As you know, in the early hours of on Sunday the 17th of May, I declared the Ebola outbreak in DRC a public health emergency of international concern, after consulting the Ministers of Health of both DRC and Uganda, and after the Africa CDC’s notification.
The outbreak is spreading rapidly.
So far, 101 cases have been confirmed in DRC, with 10 confirmed deaths.
But we know the epidemic in DRC is much larger. There are now more than 900 suspected cases and 220 suspected deaths.
This past Friday, WHO upgraded our risk assessment from high to very high at the national level.
We continue to assess the risk as high at the regional level and low at the global level.
Countries bordering DRC are at especially high risk and should take immediate action.
In Uganda, there are five confirmed cases and one death.
I appreciate the leadership of President Museveni in cancelling the Martyrs’ Day commemoration to prevent the further spread of the virus.
As you know, Martyrs’ Day attracts up to 2 million people.
I thank the governments of DRC and Uganda for their leadership of the response, which WHO is supporting, in close partnership with Africa CDC and many others.
On Friday, we convened a meeting of African health ministers on the margins of the World Health Assembly to update them and urge them to take action.
The community based interventions were underlined during the discussion, where there is trust deficit.
Together with the Africa CDC, WHO is establishing a continental Incident Management Support Team.
And we are finalizing a multi-agency Strategic Preparedness and Response Plan, aligned with the national plans of both DRC and Uganda, and with our partners.
In the IMST and the Strategic Plan, we have experience with Africa CDC in previous outbreaks.
WHO is on the ground, supporting national authorities with every pillar of the response, including contact tracing, establishing treatment centres, strengthening laboratory capacity, case management, infection prevention and control, risk communication, community engagement and more.
We have also released US$ 3.9 million from the WHO Contingency Fund for Emergencies.
Tomorrow I will be travelling to DRC with Dr Chikwe Ihekweazu, Executive Director of the WHE Health Emergencies Programme.
There are several aspects of this outbreak that make it especially challenging.
First, the delay in detecting the outbreak means that we are now playing catch-up with a very fast-moving epidemic.
We are urgently scaling up operations, but at the moment, the epidemic is outpacing us.
Second, as you know, the provinces of Ituri and North Kivu are highly insecure, with intensified fighting in recent months, causing more than 100 000 people to be newly displaced.
There is also significant distrust of outside authorities among the local population.
In the past week there have been two security incidents at health facilities.
Building trust in the affected communities is critical to a successful response, and is one of our highest priorities.
Third, there are no approved vaccines or therapeutics for Bundibugyo virus.
There have only been two previous outbreaks of Bundibugyo, in Uganda in 2007 and DRC in 2012.
Last week, WHO convened the leaders of several partner organizations under the interim Medical Countermeasures Network, to review the pipeline of vaccines, therapeutics and diagnostics.
WHO has recommended prioritizing two monoclonal antibodies to advance in clinical trials.
We are also recommending the evaluation of the antiviral obeldesivir in a clinical trial as post-exposure prophylaxis for people who are high-risk contacts.
This clinical trial is now being developed jointly with Africa CDC and the Collaborative Open Research Consortium on filovuruses.
We are also discussing with partners candidate vaccines in the development and manufacturing pipeline.
Excellencies,
We are facing an extremely serious and difficult outbreak. It will get worse before it gets better.
But we know this virus, and we know how to stop it. We have stopped every previous Ebola outbreak, and we will stop this one too.
As President Ramaphosa said, this can only be done with unity.
The question is just how quickly we can do it, and how many more lives will be lost before we do.
WHO is fully committed to working under the leadership of the Governments of DRC and Uganda, side by side with Africa CDC and all other partners.
We will not rest until we bring this outbreak under control.
Thank you once again for this opportunity, and for your leadership.
I thank you.

Friday, 22 May 2026
WHO Director-General's opening remarks at the media briefing on outbreaks of Ebola and hantavirus – 22 May 2026
22 May - Geneva
Good afternoon to everyone in the room, and good morning, good afternoon and good evening to those joining us online.
The Ebola outbreak in the Democratic Republic of the Congo is spreading rapidly.
Previously, WHO assessed the risk as high at the national and regional levels and low at the global level.
We are now revising our risk assessment to very high at the national level, high at the regional level, and low at the global level.
So far, 82 cases have been confirmed in DRC, with seven confirmed deaths.
But we know the epidemic in DRC is much larger. There are now almost 750 suspected cases and 177 suspected deaths.
The situation in Uganda is stable, with two cases confirmed in people who travelled from DRC, with one death.
The measures taken in Uganda, including intense contact tracing and cancelling the Martyrs’ Day commemoration, appear to have been effective in preventing the further spread of the virus.
An American national who was working in DRC has also been confirmed positive, and transferred to Germany for care.
We are also aware of reports today about another American national who is a high-risk contact who has been transferred to the Czech Republic.
The governments of DRC and Uganda are leading the response, with support from WHO and partners.
In addition to our national staff in DRC, so far we have deployed 22 international staff to the field, including some of our most experienced people;
And we have released US$ 3.9 million from the Contingency Fund for Emergencies.
We’re also in touch with UN humanitarian chief Tom Fletcher, and I thank him for allocating US$ 60 million to the response.
On the ground, we’re supporting national authorities with every pillar of the response, including contact tracing, establishing treatment centres, risk communication and community engagement, and more.
Together with the Africa CDC, WHO is also establishing a continental Incident Management Support Team.
In the coming days we will publish a multi-agency Strategic Preparedness and Response Plan – SPRP – aligned with the national plans of both DRC and Uganda, and with our partners.
As you know, unlike many previous Ebola outbreaks, which were caused by Zaire virus, this outbreak is caused by the Bundibugyo virus, for which there are no approved vaccines or therapeutics.
There have only been two previous outbreaks of Bundibugyo, in Uganda in 2007 and DRC in 2012.
Yesterday, WHO convened the leaders of several partner organizations under the interim Medical Countermeasures Network, to review the pipeline of vaccines, therapeutics and diagnostics.
The WHO R&D Blueprint has also convened its technical advisory group on therapeutics and recommended to prioritize two monoclonal antibodies to advance in clinical trials.
In addition, the advisory group recommended the evaluation of the antiviral obeldesivir in a clinical trial as post-exposure prophylaxis for people who are high-risk contacts.
This clinical trial is now being developed jointly with Africa CDC and the Collaborative Open Research Consortium on filovuruses.
We are also discussing with partners candidate vaccines in the development and manufacturing pipeline.
As you know, the provinces of Ituri and North Kivu in which the outbreak is occurring are highly insecure, with intensified fighting in recent months, causing more than 100 000 people to be newly displaced.
Across both provinces, around 4 million people need urgent humanitarian assistance, 2 million are displaced, and 10 million face acute hunger.
There is also significant distrust of outside authorities among the local population.
Just yesterday, there was a security incident at a hospital in Ituri, where tents and medical supplies were set on fire.
Building trust in the affected communities is critical to a successful response, and is one of our highest priorities.
We are also committed to ensuring that essential health services for the affected communities are maintained and strengthened, based on their needs.
===
Now a brief update on the hantavirus outbreak among passengers and crew on board the cruise ship MV Hondius.
Today, the Netherlands confirmed an additional case among a crew member who disembarked in Tenerife, was repatriated to the Netherlands and has been isolating since then.
There are now 12 reported cases and 3 reported deaths.
No deaths have been reported since the 2nd of May, when the outbreak was first reported to WHO.
We continue to urge affected countries to monitor all passengers and crew carefully for the remainder of the quarantine period.
More than 600 contacts continue to be followed in 30 countries, and a small number of high-risk contacts are still being located.
Once again, I thank the many countries that have cooperated in the response, and the epidemiological investigation: Argentina, Cabo Verde, Chile, Netherlands, South Africa, Spain, the United Kingdom and the European Union.
Christian, back to you.

Wednesday, 20 May 2026
WHO Director-General's opening remarks at the media briefing on Ebola outbreak in DRC and Uganda – 20 May 2026
20 May - Geneva
Good morning to everyone in the room, and hello to everybody joining us online. Thank you for joining us.
Early on Sunday, I declared a public health emergency of international concern over an epidemic of Ebola disease in the Democratic Republic of the Congo and Uganda.
This is the first time a Director-General has declared a PHEIC before convening an Emergency Committee.
I took this step in accordance with Article 12 of the International Health Regulations, after consulting the Ministers of Health of DRC and Uganda, and in view of the need for urgent action.
I determined that the situation was not a pandemic emergency, which is the new and highest classification under the amended International Health Regulations.
After declaring the PHEIC, I immediately convened an Emergency Committee under the IHR, which met yesterday and agreed that the situation is a public health emergency of international concern, but is not a pandemic emergency.
WHO assesses the risk of the epidemic as high at the national and regional levels, and low at the global level.
So far, 51 cases have been confirmed in the DRC, in the northern provinces of Ituri and North Kivu, including in the cites of Bunia and Goma – although we know the scale of the epidemic in DRC is much larger.
Uganda has also informed WHO of two confirmed cases in the capital Kampala, including one death, among two individuals who travelled from DRC to Uganda.
An American national who was working in DRC has also been confirmed positive, and been transferred to Germany.
There are several factors that warrant serious concern about the potential for further spread and further deaths.
First, beyond the confirmed cases, there are almost 600 suspected cases and 139 suspected deaths.
We expect those numbers to keep increasing, given the amount of time the virus was circulating before the outbreak was detected.
Second, the epidemic has expanded, with cases reported in several urban areas.
Third, deaths have been reported among health workers, indicating healthcare-associated transmission.
Fourth, there is significant population movement in the area.
The province of Ituri is highly insecure. Conflict has intensified since late 2025, and fighting has escalated significantly over the past two months, with over 100 000 people newly displaced.
The area is also a mining zone, with high levels of population movement that increase the risk of further spread.
And fifth, this epidemic is caused by Bundibugyo virus, a species of Ebola virus for which there are no approved vaccines or therapeutics.
In light of all these risks, I decided it was urgent to act immediately to prevent more deaths and mobilise an effective and international response.
I would like to thank the Government of DRC, the National Institute for Biomedical Research, the National Institute of Public Health and the local health authorities in the affected areas for their leadership and cooperation.
I also thank the Government of Uganda for postponing the annual Martyrs’ Day celebrations, which can attract up to two million people, because of the risk posed by the epidemic.
My thanks especially to His Excellency President Musiveni for taking this action.
WHO has a team on the ground supporting national authorities to respond. We have deployed people, supplies, equipment and funds.
To support our response, I have approved an additional US$ 3.4 million from the Contingency Fund for Emergencies, bringing the total to US$ 3.9 million.
In the absence of vaccines and therapeutics, there are many other measures countries can take to stop the spread of the virus and save lives, which the Emergency Committee has outlined in its temporary recommendations.
To say more, I’m pleased to invite the Chair of the Committee, Professor Lucille Blumberg, from the University of Pretoria in South Africa.
Professor Blumberg, thank you for your leadership at this time. Over to you.
Related links
EBOLA BUNDIBUGYO VIRUS DISEASE OUTBREAK Democratic Republic of the Congo | Uganda Weekly External Situation Report 01, Data as of 18 May 2026
Ebola disease fact sheet https://www.who.int/news-room/fact-sheets/detail/ebola-disease
Photo library: https://multimedia.who.int/CS.aspx?VP3=DamView&VBID=2AOJA4DZ7UFL&PN=1&WS=AssetManagement&FR_=1&W=1912&H=948
International Health Regulations
HEALTHNDEVELOPMENT EDITORIAL
COVID‑19 Preparedness Is Now the Shield Against Ebola: A Governance, Faith, and Community Imperative for the DRC
HEALTHNDEVELOPMENT EDITORIAL
COVID‑19 Preparedness Is Now the Shield Against Ebola: A Governance, Faith, and Community Imperative for the DRC
By His Eminence Excellency Minister Dr. Akwo Thompson Ntuba — Global Physician‑Communicator, Governance Chronicler & Editor‑in‑Chief, HealthNDevelopment
For more than three decades, my work has taken me from the clinics of Cameroon to the conference halls of Europe, from the baobab‑tree training grounds of USAID to the emergency rooms and command centers of the United States. I have stood at the crossroads of governance, faith, and public health — watching how nations rise or fall when confronted with crisis.
During COVID‑19, I served across American cities — Houston, Austin, Dallas, Detroit — helping mayors, governors, lawmakers, and community leaders build systems of preparedness. I witnessed firsthand how governance failures magnify disease, and how community trust, faith institutions, and disciplined communication can save lives.
Today, as Ebola Bundibugyo resurfaces in the Democratic Republic of Congo and Uganda, I say without hesitation:
The hard work we invested during COVID‑19 — the sleepless nights, the governance reforms, the community mobilization — is now the shield that must protect the world again.
A Crisis That Demands More Than Medicine
The WHO’s 20 May 2026 briefing confirms what many of us feared: Ebola has been circulating undetected for weeks. It has reached urban centers. It has crossed borders. It has infected health workers. It is spreading through a mining corridor marked by insecurity and displacement.
These are not merely epidemiological challenges. They are governance challenges.
As I learned during my years of COVID‑19 deployments and WHO briefings, viruses exploit weak systems, fractured leadership, and broken trust. Ebola is doing exactly that.
Governance: The Foundation of Containment
In every outbreak I have studied or responded to — from HIV to cholera to COVID‑19 — the decisive factor has always been governance.
During COVID‑19, I worked with U.S. local, state, and federal authorities to build unified command structures. I saw how a single message, a single chain of command, and a single table for decision‑making can turn chaos into coordination.
The DRC must now adopt the same architecture:
-
National Ebola Command
-
Provincial Command in Ituri and North Kivu
-
District/Health‑Zone Command
-
Faith & Community Advisory Council — a governance innovation I have championed for years
This is the model that saved lives in America. It is the model that can save lives in the DRC.
Faith Institutions: The Untapped Powerhouse of Public Health
My work has always stood at the intersection of faith and health. I have preached in churches, trained clergy, and partnered with spiritual leaders across continents. I have seen how faith institutions can calm fear, correct misinformation, and mobilize communities faster than any government ministry.
Uganda’s decision to postpone Martyrs’ Day — an event that draws nearly two million people — is a powerful example of responsible faith leadership.
But we must go further.
Faith institutions must be integrated into the Ebola response as:
-
Early‑warning surveillance nodes
-
Trusted messengers for risk communication
-
Safe and dignified burial partners
-
Providers of psychosocial and spiritual care
-
Community mobilizers in conflict‑affected zones
This is not theory. This is the model I used during COVID‑19 in immigrant communities, African diaspora churches, and U.S. cities. It works.
Community Preparedness: The Culture That Saves Lives
Preparedness is not a document. It is not a workshop. It is a culture.
My Positive Deviance work across Africa and my COVID‑19 deployments in the U.S. taught me that communities often hold the solutions long before governments arrive.
In the DRC, where displacement, mining‑zone mobility, and insecurity complicate response, community‑rooted systems are essential:
-
Community Health Action Networks
-
Door‑to‑door educators
-
Rumor‑tracking teams
-
Mining‑zone mobility monitors
-
Local radio and WhatsApp communication hubs
These are low‑cost, high‑impact interventions — the same ones that helped communities survive COVID‑19 when vaccines were scarce.
Equity and Humanitarian Access: The Moral Duty
As a physician and minister, I have always insisted that health is a moral calling.
The WHO briefing notes that more than 100,000 people have been displaced in two months. No outbreak can be controlled when health workers cannot reach the sick.
We must establish:
-
Humanitarian corridors
-
Protection for health workers
-
Negotiated access with local leaders
-
Mobile clinics for displaced populations
Ebola is not just a virus. It is a test of our humanity.
Future Preparedness: The Doctrine We Must Build Now
COVID‑19 taught the world that preparedness cannot be seasonal. It must be institutionalized.
My governance and preparedness doctrine calls for:
-
Permanent Epidemic Preparedness Councils
-
Faith‑government health compacts
-
Digital early‑warning systems
-
Preparedness curricula for youth and faith institutions
-
Community‑based surveillance networks
This is how nations build resilience. This is how Africa leads. This is how we honor the sacrifices of COVID‑19.
Conclusion: The Work Was Not in Vain
When I look back at the years of COVID‑19 work — the WHO briefings, the U.S. deployments, the community mobilization, the faith partnerships — I see clearly that none of it was wasted.
It was preparation for this moment.
Preparedness is destiny. Governance is protection. Faith is resilience. Community is survival.
And together, they form the shield the DRC — and the world — needs now.
WHO ramps up support to the Democratic Republic of the Congo’s Ebola outbreak response

WHO ramps up support to the Democratic Republic of the Congo’s Ebola outbreak response
Kinshasa—The World Health Organization (WHO) is intensifying efforts and supporting the Democratic Republic of the Congo’s government to rapidly establish and scale up critical measures to control and halt the outbreak of Ebola in the country’s north-eastern Ituri Province
Following the declaration of the outbreak on May 15, 2026, WHO acted rapidly, delivering 11.5 tonnes of vital medical supplies and equipment within 72 hours from facilities in Kinshasa and from its Regional Emergency Hubs in Dakar and Nairobi.
More than 35 experts and first responders from WHO and the Ministry of Health have been deployed to the field. Additional teams are being deployed as the response intensifies to reinforce key measures including disease surveillance for early detection; clinical care; infection prevention and control; and engaging communities to ensure public health measures are observed.
Collaboration with partner organizations and the private sector has been crucial in the timely delivery of the emergency supplies. The United Nations Organization Stabilization Mission in the Democratic Republic of the Congo (MONUSCO) has provided essential airlift support for transporting supplies from Nairobi and facilitated ground access to enhance operational effectiveness.
“The collaboration with MONUSCO has been pivotal in ensuring a swift response. Their ability to provide airlift support significantly enhances our logistics capabilities, allowing us to respond to the needs of the community effectively,” said Adama Thiam, Head of Regional Emergency Operations and Logistics at WHO Africa.
In addition, negotiations with Ethiopian Airlines enabled reprioritization of their flights to ensure urgent delivery of cargo, demonstrating the commitment of our partners to assist during this critical time.
The supplied materials include personal protective equipment, medical kits, tents, and water, sanitation and hygiene items—all crucial for preventing infection and managing cases effectively.
Additional supplies are already in transit from Kinshasa and will reach Ituri in the coming days to bolster response operations, save lives, protect frontline responders and help end the outbreak.
The outbreak is unfolding against a complex epidemiological, humanitarian and security backdrop characterized insecurity, highly mobile populations, including cross-border and trade such as mining, as well as the presence of large refugee communities.
The WHO Director-General has determined that the outbreak, caused by Ebola Bundibugyo virus, constitutes a Public Health Emergency of International Concern, requiring international coordination and cooperation for the response.
Unlike Ebola virus disease, no licensed vaccine or specific treatment exists for Bundibugyo virus disease. Research and development initiatives are being mobilized to identify and advance potential medical countermeasures. Response strategies will rely heavily on comprehensive public health measures, including supportive care, early case detection, stringent infection prevention and control protocols, rigorous contact tracing, safe burial practices, and deep community engagement.
The outbreak is the Democratic Republic of the Congo’s 17th since the virus was first identified in 1976. The previous one was an outbreak of Ebola virus disease that ended in December 2025.
WHO convenes partners to strengthen Ebola response in the Democratic Republic of the Congo

WHO convenes partners to strengthen Ebola response in the Democratic Republic of the Congo
Brazzaville/Kinshasa — As part of efforts to support the ongoing response to the Ebola outbreak in the Democratic Republic of the Congo, the World Health Organization convened governments, partners and technical agencies to align response priorities and reinforce preparedness across affected and neighbouring countries.
The outbreak has affected several health zones in Ituri Province, including Mongbwalu, Rwampara and Bunia, where health authorities are responding to confirmed cases, suspected deaths and infections among healthcare workers. The evolving situation, combined with insecurity and population mobility linked to mining and trade activities, continues to complicate response efforts and increase the risk of wider transmission.
WHO is reinforcing support to national and provincial authorities through deployment of technical expertise and emergency supplies to strengthen surveillance, case investigation, infection prevention and control, laboratory capacity, clinical care and community engagement activities.
Additional specialists in epidemiology, logistics, laboratory diagnostics, clinical care and community engagement are being mobilized to support frontline teams and help strengthen outbreak control measures in affected areas.
“Clear coordination mechanisms at provincial level will be critical to help partners rapidly align and mobilize support where it is most needed,” said Dr Mir Rahimzai, FHI 360.
Participants highlighted the importance of strong community engagement and coordinated operational approaches to strengthen public trust and support response efforts in affected communities.
The meeting brought together more than 220 participants from WHO, Ministries of Health, Africa CDC, UN agencies, humanitarian organizations, research institutions and partners following the official declaration of the outbreak by the Government of the Democratic Republic of the Congo on 15 May.
Partners are expanding response activities on the ground. Médecins Sans Frontières is supporting patient isolation and infection prevention and control activities in Mongbwalu and Bunia, while additional teams and supplies are being mobilized for deployment to the Democratic Republic of the Congo and Uganda.
The World Food Programme confirmed readiness to support airlift operations between Kinshasa and Bunia to facilitate rapid delivery of emergency supplies and equipment to affected areas.
The International Organization for Migration is supporting preparedness and surveillance activities at points of entry and along key cross-border corridors linking the Democratic Republic of the Congo, Uganda and South Sudan.
“Cross-border population movement remains a key factor in this outbreak. IOM teams are already supporting preparedness and surveillance efforts on the ground in the Democratic Republic of the Congo and Uganda,” said Dr Jerry Geoffrey Mtike, IOM.
Countries across the region are also strengthening readiness measures to reduce the risk of further spread. Zambia highlighted vulnerabilities linked to mining and trade corridors and identified diagnostic capacity, sample transport systems and cross-border surveillance among key preparedness priorities.
Dr Francis Kasolo, WHO Representative, Ethiopia, underscored the importance of strengthening preparedness beyond land borders, including air travel routes, and called for pre-positioning of essential supplies in high-risk countries.
WHO is also scaling up regional readiness activities, including deployment of supplies, laboratory coordination and development of a multi-country Strategic Preparedness and Response Plan with partners. Priority countries are being supported to strengthen emergency coordination, border surveillance, healthcare worker training and contingency planning to enhance readiness and reduce the risk of further spread.
CDC Mobilizes International Response Following Ebola Disease Outbreak in DRC and Uganda

CDC Mobilizes International Response Following Ebola Disease Outbreak in DRC and Uganda
The Centers for Disease Control and Prevention (CDC) has mobilized response activities following confirmation of an Ebola outbreak in Ituri Province, Democratic Republic of the Congo (DRC) and cases in Uganda. Through existing relationships with the DRC and Uganda Ministries of Health, CDC was notified of the ongoing outbreak as soon as cases were confirmed and have been actively working to support needs. Last night, the WHO followed this notification with a declaration of a public health emergency of international concern with regard to this epidemic of Ebola disease caused by the Bundibugyo (Bun-dee-BOO-joh) virus, a species of orthoebolavirus, in the DRC and Uganda.
At this time, the risk to the American public remains low. Ebola virus spreads through direct contact with the bodily fluids of an infected person and does not spread through casual contact or air. CDC continues to closely monitor the situation and has systems in place to detect and respond rapidly to potential public health threats.
The CDC's Country Offices in the DRC and Uganda have been coordinating across the U.S. Government, Ministries of Health, other members of the USG, and international partners to support response operations, including surveillance, laboratory diagnostics, infection prevention and control, and other outbreak containment efforts.
CDC is also supporting interagency partners who are actively coordinating the safe withdrawal of a small number of Americans who are directly affected by this outbreak.
The affected areas of Ituri Province are logistically challenging regions in eastern DRC, with limited transportation infrastructure, difficult terrain, and ongoing security concerns that can complicate access for response teams and medical personnel. CDC has extensive experience and some of the world's foremost experts in supporting Ebola response operations in the region and remains committed to protecting global health security. Most recently, the CDC responded to an Ebola outbreak in the DRC that ended in December 2025.
To date, there are reports of 10 confirmed cases, 336 suspected cases including 88 deaths in DRC, and 2 confirmed cases including 1 death in Uganda. Cases and death numbers are subject to adjustment as the situation evolves. This marks the DRC's 17th Ebola virus outbreak since 1976, and its second outbreak of Bundibugyo virus.
For immediate release: May 17, 2026
For the latest updates and public health information, visit Ebola Disease: Current Situation.
Related Pages
- Releases
- CDC Provides Update on Hantavirus Outbreak Linked to M/V Hondius Cruise Ship
- Transcript - Update on Ebola Outbreak in the Democratic Republic of the Congo and Uganda, 5/18/2026
- Transcript - Update on Ebola Outbreak in the Democratic Republic of the Congo and Uganda, 5/17/2026
- Transcript - Update on CDC's Hantavirus Response 5/15/2026
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES
Whether diseases start at home or abroad, are curable or preventable, chronic or acute, or from human activity or deliberate attack, CDC’s world-leading experts protect lives and livelihoods, national security and the U.S. economy by providing timely, commonsense information, and rapidly identifying and responding to diseases, including outbreaks and illnesses. CDC drives science, public health research, and data innovation in communities across the country by investing in local initiatives to protect everyone’s health.
Statement on the escalating Ebola outbreak in the DRC and Uganda

The World Council of Churches is deeply concerned by the suffering caused by the escalating Ebola outbreak in the Democratic Republic of Congo and Uganda, which the World Health Organization (WHO) has declared a public health emergency of international concern, with hundreds of suspected infections and many deaths reported.
This outbreak is unfolding in contexts already burdened by poverty, fragile health systems, food insecurity, displacement and the long-term impacts of conflict. Such socio-economic vulnerabilities heighten exposure to disease, limit access to timely care, and undermine the ability of individuals and communities to adopt preventive measures. These conditions not only accelerate the spread of Ebola but also increase the risk of wider epidemics and future pandemics, reminding us that health crises are deeply intertwined with issues of justice, equity and human dignity.
In this time of fear and uncertainty, we affirm that church and community leaders have a vital role as trusted neighbours: to stay alert, to follow and disseminate accurate public health guidance, and to counter misinformation with clear, compassionate and trustworthy information that protects life.
We call on governments, international agencies, churches and civil society to cooperate across borders, to share treatments, technologies and financial resources so that the most affected communities are not left behind, and to ensure safe and unhindered access for health workers and humanitarian actors. We note with grave concern that, according to the WHO, there is currently no approved vaccine or therapeutics for the Bundibugyo strain of Ebola driving this outbreak. In this context, it is imperative to strengthen preventive measures and to intensify efforts to develop effective therapies and vaccines that are timely, affordable and accessible to all.
We further urge that investments in outbreak response be matched by sustained commitments to strengthen primary health care, disease surveillance systems, and community-based health education, particularly in underserved and high-risk areas.
We therefore urge all parties to ongoing conflicts in the region to agree to an immediate cessation of hostilities, to respect international humanitarian law, and to create secure corridors for medical response, community education and care, recognising that peace and health are inseparably linked.
The WCC calls on communities worldwide to accompany the most vulnerable—the sick and their families, health workers, displaced people, women and children at risk, and communities already scarred by violence and poverty—through persistent prayer, courageous advocacy and concrete acts of solidarity.
In this shared global responsibility, we reaffirm that solidarity must extend beyond emergency response to addressing the root causes of vulnerability, including inequality, marginalization and lack of access to essential services, so that communities are better protected against future health crises.
Rev. Prof. Dr Jerry Pillay
General Secretary
World Council of Churches